

Alexandre Marochi de Castro1; Luísa Fernandes Schenato1; Maurício Marcondes Ribas2
DOI: 10.5935/2595-170X.20250022
ABSTRACT
INTRODUCTION: Brazil has a rate of 1 million burns annually, the majority occurring at home, affecting children mainly. Additionally, the social isolation during the COVID-19 pandemic contributed to children staying home, which could be a factor that increased the incidence of burns.
OBJECTIVE: To compare the epidemiological profile of pediatric burn patients during social isolation and after the relaxation of sanitary measures, thus assessing the impact of social isolation on this population.
METHODS: Retrospective cross-sectional observational study, analyzing 410 electronic medical records (March 2020 to December 2022) of pediatric patients treated at the Evangélico Mackenzie University Hospital (EMUH). The variables analyzed qualitatively included age, sex, burn etiology, accident location, burn depth, injury severity, type of treatment, length of hospital stay, and prognosis. Ten records from January and February 2020 were excluded, and the remaining sample was divided into two groups: 252 treated during social isolation and 148 after the relaxation of sanitary measures.
RESULTS: Of the 410 patients, 133 were in 2020, 129 in 2021, and 148 in 2022. There was no significant difference in the annual incidence during or after the pandemic. There were no significant differences in the epidemiological profile of the patients, treatment type, or prognosis, only in the degree and severity of the burns.
CONCLUSIONS: The pandemic did not affect the number of pediatric burn cases treated, only the severity and depth of the injuries. However, there was no impact on the treatment or prognosis of the patients.
Keywords: Burns. Pediatrics. COVID-19. Epidemiology.
RESUMO
INTRODUÇÃO: O Brasil apresenta uma taxa de 1 milhão de queimaduras anualmente, a maioria ocorre em casa, afetando principalmente crianças. Além disso, o isolamento social durante a pandemia de covid-19 contribuiu para que as crianças permanecessem em casa, fator que poderia aumentar a incidência de queimaduras.
OBJETIVO: Comparar o perfil epidemiológico dos pacientes pediátricos queimados durante o isolamento e após a liberação das medidas sanitárias, avaliando assim o impacto do isolamento na população.
MÉTODO: Estudo observacional transversal retrospectivo, que analisou 410 prontuários eletrônicos (março/2020 e dezembro/2022) dos pacientes pediátricos atendidos no Hospital Universitário Evangélico Mackenzie (HUEM). As variáveis analisadas qualitativamente incluíram idade, sexo, etiologia da queimadura, local do acidente, profundidade da queimadura, gravidade da lesão, tipo de tratamento, tempo de internação e prognóstico. Dez prontuários de janeiro e fevereiro de 2020 foram excluídos e a amostra restante foi dividida em dois grupos: 252 atendidos durante o isolamento social e 148 após o relaxamento das medidas sanitárias.
RESULTADOS: Dos 410 pacientes, 133 foram atendidos em 2020, 129 em 2021 e 148 em 2022. Não houve diferença significativa na incidência anual durante ou após a pandemia. Não houve diferença significativa no perfil epidemiológico dos pacientes, tipo de tratamento ou prognóstico, apenas no grau e gravidade das queimaduras.
CONCLUSÕES: A pandemia não afetou no número de casos de queimaduras pediátricas no serviço, apenas na gravidade e profundidade das lesões. Entretanto, isso não impactou no tratamento ou prognóstico dos pacientes.
Palavras-chave: Queimaduras. Pediatria. COVID-19. Epidemiologia.
INTRODUCTION
COVID-19 caused the largest hospital collapse in Brazil and the world, the according to the Oswaldo Cruz Foundation, furthermore, people were isolated at home during the period, leading to an increase in domestic accidents, such as burns1,2. This was due to higher alcohol use for sanitation, more cooking at home, and difficulty supervising children during the home office1,3.
Burns generally occur in domiciliary ambient (70%), reaching 1 million people, annually, of this 40,000 needs hospitalization, according Brazilian Burn Society4. Burns are the third leading cause of accidental death in children worldwide5.
A 2013-2014 study at Evangélico Mackenzie University Hospital (EMUH) showed that pediatric burns mainly affect boys, with 42% in children under 1 year old. The most common cause of burns is scalding6.
Burns can be classified as chemical, physical or thermal, affecting the epidermis, dermis, cutaneous appendages, and underlying tissues7. For better management, burns are categorized by skin layer, extent of injury, and etiology8.
First-degree burns affect the epidermis with local edema and hyperemia8. Second-degree burns, more common, cause dermal necrosis and blister formation7,8. Third-degree burns involve full-thickness skin damage, causing painless, dry wounds and necrosis due to nerve and vascular destruction7.
Burn extent is assessed in second- and third-degree burns, using methods like the Rule of Nines (modified for children) and the Lund-Browder Chart, which is more accurate, because it accounts for age and anatomical area7-9. Additionally, has a practice rule, that the hand surface is 1% of body surface8.
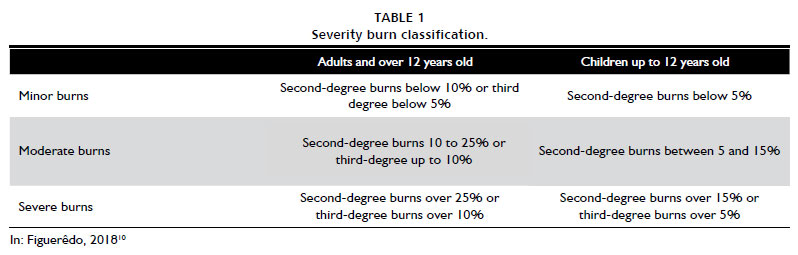
Burn severity is classified as small, medium or large burns. According to the table (Table 1). Additionally, large burns are defined as second- or third-degree burns in the perineum, or third-degree burns affecting the hands, feet, face, neck, or axilla10.
Under analysis by DATASUS, there were 7,232 hospitalizations of children under 10 years of age in Brazil during 2021 (pandemic period), because of burns11.
A Chinese study, conducted at the Department of Burn Surgery at the First Hospital of Jilin University, with 489 pediatric patients burned, 335 treated pre-COVID-19 pandemic and 154 during isolated (pandemic period). It was realized that during COVID-19 period the number for hospitalizations decreased, although the severity burns and complications increased, associated to the delay in hospital visits, due to the overload healthcare system. Furthermore the scalds burn remained the main reason for the burn hospitalization12.
This study aims to compare the epidemiological profile of pediatric burn patients during the social isolation period and after the easing of health measures, assessing the impact of isolation on this population.
METHODS
A retrospective observational cross-sectional study, approved by the ethics committee (CAAE: 70088823.4.0000.0103), was conducted by reviewing electronic medical records of pediatric patients (under 18 years old) treated for second- and third-degree burns at the Evangélico Mackenzie University Hospital (EMUH) - referral hospital for burns in the state of Paraná, between 2020 and 2022.
The data analyzed are the patients that receive hospital discharge or died, thus did not active in service, then there was a waiver of the Free and Informed Consent Form. And all authors declare that they have no interest conflicts.
Initially, 635 medical records were reviewed, excluding the incomplete, duplicate or active data, resulting in 410 records. Subsequently, from January and February 2020 were excluded, because it is before COVID-19 pandemics. The variables analyzed included age, sex, etiology, burn degree and severity, type of treatment, length of hospital stay and prognosis.
The sample was divided into two groups: the social isolation period (March 2020 to December 2021) and after the release of sanitary measures (2022), Although the release of sanitary measures occurred progressively in Brazil, this year was marked by the start of the biggest reopening in the country since the beginning of the pandemic. The Student's T-test was used for statistical analysis, and the Chi-Square test was applied to compare the epidemiological profile, with a 95% confidence interval. All data were tabulated in Excel.
RESULTS
Of the 410 medical records analyzed (January 2020 to December 2022), 133 burns occurred in 2020 (32%), of which 10 were excluded because they corresponded to January and February 2020, prior to the pandemic. 129 consultations occurred in 2021 (31%) and 148 in 2022 (36%), with no statistically significant difference between the incidences (p=0.4799).
From March 2020 to December 2022, 400 medical records were analyzed. Of these, 252 were from the social isolation period (March 2020 to December 2021) and 148 were after the liberation of sanitary measures (2022).
Regarding sex, during the isolation period, 60% of the patients were male and 40% were female. After the liberation of sanitary restrictions, the distribution was 58% and 42%, respectively, with no significant difference (p=0.7217).
The most affected age group in both periods were children under 3 years old, accounting for more than 50% in the two periods. There was no significant difference between the periods (p=0.2065).
Hot liquids were the primary etiology (62% in both periods), followed by explosions, 15% during the pandemic and 11% after the liberation of sanitary measures (p=0.4955). Most accidents occurred at home, with 76% during isolation and 77% after (p=0.5684). None of the variables showed a significant difference.
The degree of burns showed a significant difference between the periods (p=0.0003), the depth was divided in three groups: second-degree burn, second + third - degree burn, third-degree burn.
Second-degree burns accounted for 48% during social isolation and 51% after the liberation of sanitary measures.
Second + Third-degree represented 39% in 2020-2021 and 28% in 2022. Third-degree burns accounted for 7% and 18%, respectively, during the pandemic and after the relaxed of health measures.
About this topic 7% of medical records were incompletely filled during the isolation period and 2% after the release of sanitary measures.
A significant difference was also observed in the severity of burns (p=0.0048). During the pandemic, 10% were classified as minor burns, 12% as moderate and 71% as severe burns. Additionally, 8% of the medical records lacked this information. After the liberation of sanitary measures, 17% were classified as minor burns, 16% as moderate burns, and 66% as severe burns, with 1% of the records incomplete.
Analyzing both during social isolation and after the liberation of sanitary measures, more than 90% of patients in both periods had a hospital stay, remaining for less than 30 days, with no significant difference between the periods (p=0.3380).
Regarding prognosis, most patients showed improvement, with or without aesthetic sequelae, with no significant difference between the periods. Of the entire sample, there were 6 deaths, 3 during isolation and 3 after (p=0.5373).
DISCUSSION
The boys were the main gender affected in this study, the literature confirms this finding, for example, a study realized in Londrina University Hospital (LUH), that analyzed 177 patients, 67% were men13. This is more related to the greater exposure of males to environments that cause burns13.
In our study, the most affected age group was children up to 18 months, representing 29% (social isolation) and 39% (release of sanitary measures). In the study carried out at the Children's Hospital, Milan, during the COVID-19 pandemic and after the release of sanitary measures (January 2020 to June 2022), the highest incidence was between 0 and 4 years old14. The literature indicates that the highest incidence of childhood burns is between 0 and 5 years old5,11,13,14.
The main etiology was scalding with hot liquids (62%) in both periods, followed by explosions (15% - social isolation and 11% - release of sanitary measures). The studies confirms that burns caused by hot liquids are the most common, representing, for example, 79% of the patients in the study in Milan14.
The home environment was identified as the predominant location of accidents, exceeding 70% in the COVID-19 pandemic or after, despite this, no significant difference was seen in the periods. The hypothesis that social isolation would increase the number of burn cases was not confirmed, possibly due to families' fear of seeking medical care during the pandemic or the overload of the health system13,15.
Regarding the depth burns, after the release sanitary measures the second-degree increased, furthermore the second + third-degree decreased in this period, compared to the pandemic period. Importantly highlighted that 7% of the medical records during the COVID-19 pandemic did not contain this information of depth.
In addition to the depth of the burn, the severity of the injuries also showed significant differences. During the pandemic, there were more severe burns, and after the release of health measures, moderate and minor burns prevailed. And 8% of the medical records did not contain information on severity, during the COVID-19 pandemic. The increase in the severity of the injuries can be explained by the reduction in supervision of children during the isolation period, due to home office, and incomplete medical records may be associated with hospital overload. The greater severity of burns in study may also be related to hospital overload, with the reference hospital, like EMUH, only receiving severe burns1,16.
In other study realized in the EMUH, with 470 burns patients, which compared the epidemiologic profile of burn patients of all age groups before (2019) and during the COVID-19 pandemic (March to August/2020), realized a significant increase in the severity of burns in pediatric patients, during the pandemic16. In a study performed in China, with a sample of 489 patients, compared before pandemic (July/2017 and December/2019) with a pandemic group (January/2020 to June/2022) it was found an increase in the severity of burns only in pediatric patients12.
As for treatment, more than 90% of the patients were hospitalized in both periods, but in most cases, this did not exceed 30 days. Despite the changes in the severity of the injuries, the treatment pattern and length of hospital stay remained similar that observed in previous studies in the literature17.
The prognosis of the patients did not undergo significant changes, more than 80% of the patients, in both periods, improved, with or without aesthetic sequelae. Had 6 deaths in the analyzed period, 3 during COVID-19 pandemic and 3 after. This suggests that the treatment protocol was effective and maintained the prognosis even in an atypical period.
As the EMUH is the referral hospital for burns victims, the data may be biased, because the service receive more critically patients, compared to other services of medium and low complexity, especially in pandemic, that the reference hospital stayed rearguard for these cases. In despite it, the hospital also attends many minor burns.
CONCLUSIONS
The results suggest that, despite the increased risk of burns in the home environment, social isolation did not contribute to a rise in the incidence of pediatric burn cases treated at EMUH. The pandemic affected the severity and depth of the burns treated, but there were no significant changes in the management, hospitalization, or prognosis of the burned children.
REFERENCES
1. Gobetti JSC, Zraik MB, Afornali CB, Goveia CHM, Naufel Junior CR, Coelho GA, et al. Comparative analysis of the trauma care profile before and during the COVID-19 pandemic: a cross-sectional study in a tertiary university hospital. Rev Col Bras Cir. 2023;50:e20233449.
2. Ortíz-Barrios M, Jaramillo-Rueda N, Gul M, Yucesan M, Jiménez-Delgado G, Alfaro-Saíz JJ. A Fuzzy Hybrid MCDM Approach for Assessing the Emergency Department Performance during the COVID-19 Outbreak. Int J Environ Res Public Health. 2023;20(5):4591.
3. Pan R, Santos PMFD, Resende IL, Nascimento KGD, Adorno J, Cunha MTRD, et al. Domestic burns that occurred during the COVID-19 pandemic in Brazil: a descriptive cross-sectional study. São Paulo Med J. 2023;141(1):4-11.
4. Nascimento LKA, Barreto JM, Costa ACSM. Análise das variáveis grau e porte da queimadura, tempo de internação hospitalar e ocorrência de óbito em pacientes admitidos em uma Unidade de Tratamento de Queimados. Rev Bras Queimaduras. 2013;12(4):256-9.
5. Rigon AP, Gomes KK, Posser T, Franco JL, Knihs PR, Souza PA. Perfil epidemiológico das crianças vítimas de queimaduras em um hospital infantil da Serra Catarinense. Rev Bras Queimaduras. 2019;18(2):107-12.
6. Morais IH, Daga H, Prestes MA. Crianças queimadas atendidas no Hospital Universitário Evangélico de Curitiba: perfil epidemiológico. Rev Bras Queimaduras. 2016;15(4):256-60.
7. Jenkins-Hopkins JM. Doenças Associadas a Agente Físicos: Calor, Frio, Radiação e Trauma. In: Elder DE, Elenitsas R, Johnson Junior BL, Murphy GF, Xu X, eds. Lever: Histopatologia da Pele. 10ª ed. Rio de Janeiro: Guanabara Koogan; 2011. p. 327-30.
8. Bravo BSF, Vale ECS, Serra MC. Queimaduras. In: Azulay RD, Azulay DR, Abulafia LA. Dermatologia. 7ª ed. Rio de Janeiro: Guanabara Koogan; 2017. p. 44-50.
9. Nazário ON, Leonardi DF, Nitschke CAS. Queimaduras: eventos agudos em situações clínicas. Florianópolis: Universidade Federal de Santa Catarina; 2014.
10. Figuerêdo AA. Avaliação da regra dos noves, lund browder e análise digital [Dissertação de mestrado]. Salvador: Escola Bahiana de Medicina e Saúde Pública; 2018.
11. Brasil. Ministério da Saúde. DATASUS. Tabnet. Brasília: Ministério da Saúde; 2021.
12. Zhao J, Shi K, Zhang N, Chen X, Yu J. The changing pattern of pediatric burns in a territory burn center before and during the COVID-19 pandemic in China: A retrospective study. J Tissue Viability. 2024;33(2):185-9.
13. Takino MA, Valenciano PJ, Itakussu EY, Kakitsuka EE, Hoshimo AA, Trelha CS, et al. Perfil epidemiológico de crianças e adolescentes vítimas de queimaduras admitidos em centro de tratamento de queimados. Rev Bras Queimaduras. 2016;15(2):74-9.
14. Pelizzo G, Lanfranchi G, Pantaloni M, Camporesi A, Tommasi P, Durante E, et al. Epidemiological and Clinical Profile of Pediatric Burns in the COVID-19 Era: The Experience of a Reference Center. Children (Basel). 2022;9(11):1735.
15. Biscegli TS, Benati LD, Faria RS, Boeira TR, Cid FB, Gonsaga RA. Profile of children and adolescents admitted to a Burn Care Unit in the countryside of the state of São Paulo. Rev Paul Pediatr. 2014;32(3):177-82.
16. Melquíades da Rocha BF, Bochnia MF, Ioris RA, Damin R, de Araujo Santos Nigro MV, Nisihara RM. The impact of social isolation by COVID-19 on the epidemiological and clinical profiles of the burn patients. A retrospective study. Burns. 2022;48(4):976-83.
17. Dalla-Corte LM, Fleury BAG, Huang M, Adorno J, Modelli MES. Perfil epidemiológico de vítimas de queimaduras internadas em uma unidade no Distrito Federal do Brasil. Rev Bras Queimaduras. 2019;18(1):10-5.
Recebido em
4 de Fevereiro de 2025.
Aceito em
20 de Outubro de 2025.
Local de realização do trabalho: Faculdade Evangélica Mackenzie do Paraná, Curitiba, PR, Brasil.
Conflito de interesses: Os autores declaram não haver.
![]() © 2026 Todos os Direitos Reservados
© 2026 Todos os Direitos Reservados
 Inglês PDF
Inglês PDF Imprimir
Imprimir
 Enviar este artigo por email
Enviar este artigo por email
 Como citar este artigo
Como citar este artigo
 Enviar um comentário
Enviar um comentário
 Mendeley
Mendeley
 Pocket
Pocket
