

Fabrizia Silva Moraes Alves; Edilane Voss; Annelene Boaventura; Marilda Casela; Valnélia Fraga da Silva; Marcus Vinícius V S Barroso; Nilmar G Bandeira
DOI: 10.5935/2595-170X.20250029
ABSTRACT
OBJECTIVE: To characterize antibiotic (ATB) consumption, microbiota, and antimicrobial sensitivity profiles in a Burn Treatment Center (CTQ, from Portuguese Centro de Tratamento de Queimados) at the State General Hospital in Bahia, Brazil.
METHODS: This cross-sectional study examined infection-causing pathogens and antibiotic consumption, expressed as defined daily doses (DDD), in both the CTQ ward (CTQ-A) and the Intensive Care Unit (UAC).
RESULTS: A total of 214 bacterial isolates were identified between January 2022 and May 2023: 92 from CTQ-A and 122 from UAC. In CTQ-A, 43.5% of isolates were Gram-positive compared to 17.2% in UAC. The most prevalent pathogens in CTQ- A were Staphylococcus aureus (29%), Pseudomonas aeruginosa (17.4%), coagulase-negative staphylococci (13%), Serratia marcescens (10%), Klebsiella pneumoniae and Acinetobacter baumannii (8.7% each). In UAC, dominant isolates were A. baumannii (25.4%), P. aeruginosa (16.4%), S. marcescens and K. pneumoniae (12.3% each), followed by S. aureus (9%). Multidrug-resistant organisms accounted for 50% of CTQ-A and 73% of UAC isolates. Among Enterobacterales, extended-spectrum beta-lactamase production was detected in 54% of CTQ-A and 62% of UAC isolates, whereas carbapenem resistance rates were 25% and 53%, respectively. Methicillin-resistant S. aureus occurred in 50% of CTQ-A and 66.7% of UAC isolates. Meropenem, tigecycline, piperacillin/tazobactam, teicoplanin, and polymyxin B were the most prescribed ATBs in UAC. In CTQ-A, the most used were meropenem, piperacillin/tazobactam, teicoplanin, and tigecycline.
CONCLUSIONS: Despite differences in pathogens and resistance profiles between units, the antibiotics most consumed in both were meropenem, piperacillin/tazobactam, teicoplanin, and tigecycline.
Keywords: Anti-Bacterial Agents. Infections. Critical Care. Burns. Drug Resistance.
RESUMO
OBJETIVO: Caracterizar o consumo de antibióticos (ATB), a microbiota e os perfis de sensibilidade antimicrobiana em um Centro de Tratamento de Queimados (CTQ) do Hospital Geral do Estado da Bahia, Brasil.
MÉTODOS: Estudo retrospectivo observacional que avaliou microrganismos causadores de infecções e o consumo de antibióticos, expresso em doses diárias definidas (DDD), tanto na enfermaria do CTQ (CTQ-A) quanto na Unidade de Terapia Intensiva (UAC).
RESULTADOS: Entre janeiro de 2022 e maio de 2023, foram identificados 214 isolados bacterianos: 92 no CTQ-A e 122 na UAC. No CTQ-A, 43,5% dos isolados eram Gram-positivos, comparados a 17,2% na UAC. Os patógenos mais prevalentes no CTQ-A foram Staphylococcus aureus (29%), Pseudomonas aeruginosa (17,4%), estafilococos coagulase-negativos (13%), Serratia marcescens (10%) e Klebsiella pneumoniae e Acinetobacter baumannii (8,7% cada). Na UAC, predominaram A. baumannii (25,4%), P. aeruginosa (16,4%), S. marcescens e K. pneumoniae (12,3% cada), seguidos de S. aureus (9%). Microrganismos multirresistentes representaram 50% dos isolados no CTQ-A e 73% na UAC. Entre enterobactérias, a produção de beta-lactamase de espectro estendido foi detectada em 54% dos isolados do CTQ-A e 62% da UAC; já a resistência a carbapenêmicos foi de 25% e 53%, respectivamente. S. aureus resistente à meticilina ocorreu em 50% no CTQ-A e em 66,7% na UAC. Os antibióticos mais prescritos na UAC foram meropenem, tigeciclina, piperacilina/tazobactam, teicoplanina e polimixina B. No CTQ-A, destacaram-se meropenem, piperacilina/tazobactam, teicoplanina e tigeciclina.
CONCLUSÕES: Apesar das diferenças nos perfis de resistência entre as unidades, meropenem, piperacilina/tazobactam, teicoplanina e tigeciclina foram os antibióticos mais utilizados em ambas.
Palavras-chave: Agentes Antibacterianos. Infecções. Cuidados Críticos. Queimaduras. Resistência a Medicamentos.
INTRODUCTION
Infection is the leading cause of morbidity and mortality in burn patients. Hence antimicrobials are the primary class of drugs used in the treatment of patients with burns1. However, excessive use of antimicrobials can lead to the emergence of multi-resistant bacteria, making it difficult to treat infections in the near future. The main rationale for administering antibiotics (ATBs) is to control the high risk of infection and sepsis, which are the leading causes of morbidity and mortality2. Effective infection prevention and control are essential to improve patient outcomes and reduce the misuse of antimicrobials.
Although burn profiles and microbial patterns vary across specialized care units, the most frequently implicated and prevalent bacteria include Pseudomonas aeruginosa, Serratia marcescens, Acinetobacter baumannii, and Staphylococcus aureus3. We were unable to identify studies on antibiotic consumption in specialized burn units in Brazil. Thus, raising questions: what constitutes the appropriate consumption? How long should the treatment time be? What is the indication for antibiotic prophylaxis in this population?
Antimicrobial selection must be individualized and guided by the patient's colonizing flora as well as the epidemiological profile of the burn unit4. In specific cases, tissue biopsy with microbiological analysis is required5-7. Since 2019, an active microbiological surveillance system has been implemented at the Burn Treatment Center (CTQ, from the Portuguese Centro de Tratamento de Queimados) in Salvador, Bahia, Brazil.
This system is designed to monitor all pathogens responsible for infections in hospitalized patients, characterize their antimicrobial susceptibility profiles, and track changes throughout hospitalization. The data generated through this surveillance have been instrumental in developing treatment protocols specifically tailored for this burn units. Taking account of this surveillance, this study focuses on evaluating antibiotic consumption in the burn unit.
OBJECTIVES
To report the most prescribed antimicrobials in the unit and asses whether their consumption is adequate based on the unit's pathogen data and resistance profile.
METHODS
This retrospective observational study was conducted using medical records from January 2022 to May 2023. Data were collected from both the intensive care unit (UAC) and the general burn ward (CTQ-A) of Hospital Geral do Estado (HGE), a regional reference center for burn care. Data collection was based on medical prescriptions and complemented with information provided by the Hospital Infection Control Service (Serviço de Controle de Infecção Hospitalar, SCIH) and the unit's Clinical Pharmacy. All patients admitted to the unit during the study period were included.
Antimicrobials were assessed according to the prescribed agent and defined daily dose (DDD) calculations. Susceptibility profiles were obtained through the active microbiological surveillance program. Data were compiled using Epi Info version 7.2.5 (Centers for Disease Control and Prevention, CDC).
Patient-days refer to the unit of measurement representing care provided to a hospitalized patient over a 24-hour period. The total number of patient-days during a given period represents the sum of all hospitalized patients per day.
The drug's daily dose (DDD) represents the presumed average maintenance dose per day of a drug when used for its main therapeutic indication. To calculate DDDs, the monthly consumption of each antibiotic was first converted to grams (g), and then expressed in terms of its standardized daily dose.
To calculate the standardized rate of antimicrobial consumption, the following formula was used: DDD per 1,000 patient-days = (Total amount of drug used in grams) ÷ (DDD × Total patient-days) × 1,000; where A = total antimicrobial consumed (in grams); B = standard daily dose of the antimicrobial (in grams); P = total number of patient-days during the surveillance month. This study was approved by Plataforma Bahia and the Institutional Research Ethics Committee (approval number: 5.494.951). The ethics committee waived the requirement for informed consent due to the retrospective nature of the study.
RESULTS
During the study period, 765 patients were admitted in CTQ-A and 211 patients were admitted in UAC, which corresponds to 6,122 patient-day in CTQ-A and 1,901 in UAC. The rates of healthcare-associated infections were 6.8% in the CTQ-A group and 27.2% in the UAC group.
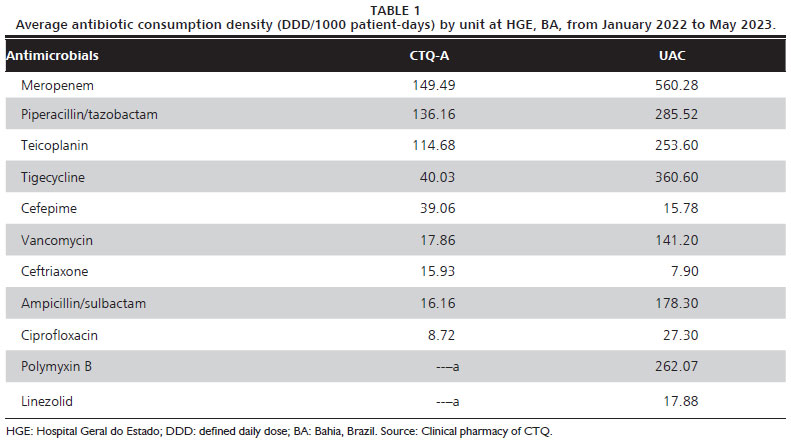
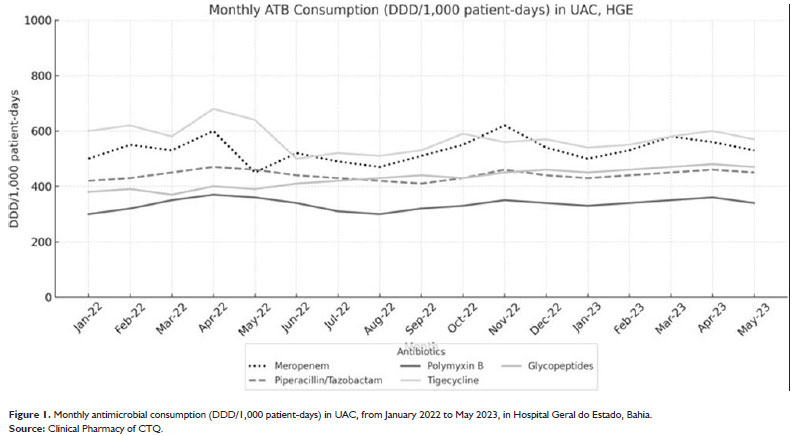
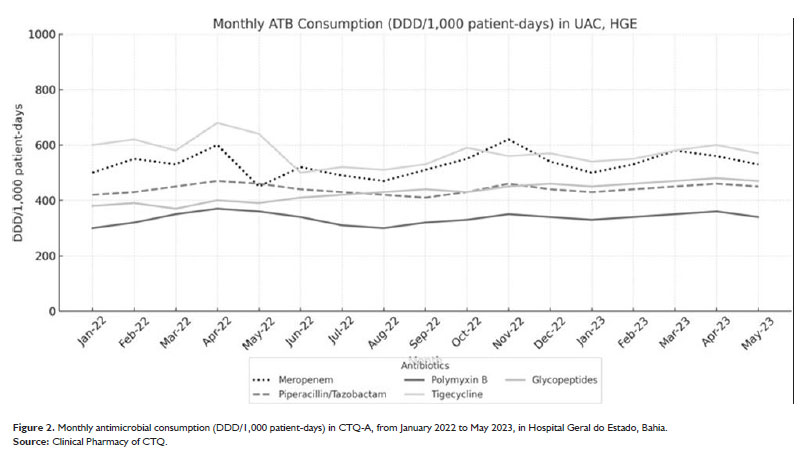
The most frequently prescribed ATBs in the UAC were Meropenem, Tigecycline, Piperacillin/tazobactam, Teicoplanin, Polymyxin B, Ampicillin/sulbactam, Vancomycin, Ciprofloxacin, Linezolid, Cefepime, and Ceftriaxone. In the CTQ-A the most prescribed ATBs were Meropenem, Piperacillin/tazobactam, Teicoplanin, Tigecycline, Cefepime, Vancomycin, Ceftriaxone, Ampicillin/sulbactam, and Ciprofloxacin. Table 1 displays the antibiotic consumption density, expressed as defined daily doses per 1,000 patient-days (DDD/1000) for each unit. The monthly consumption trends of the most frequently prescribed antimicrobials in UAC and CTQ-A are illustrated in Figures 1 and 2, respectively.
The data from the microbiology surveillance of the unit during the period showed a total of 214 microorganisms; with 122 isolated from UAC and 92 isolated from the general ward (CTQ-A).
The microbiota differed between the two units: in CTQ-A, 43.5% of the isolates were Gram-positive, whereas this proportion decreased to 17.2% in the UAC. The most prevalent pathogens in CTQ-A were S. aureus (29.0%), P. aeruginosa (17.4%), coagulase-negative staphylococci (CoNS) (13.0%), S. marcescens (10.0%), Klebsiella pneumoniae and A. baumannii (8.7%), followed by Enterobacter spp., Escherichia coli, Proteus mirabilis, and Enterococcus spp. (each 3.3%). In the UAC, the leading pathogens included A. baumannii (25.4%), P. aeruginosa (16.4%), S. marcescens and K. pneumoniae (each 12.3%), S. aureus (9.0%), E. coli (6.6%), Enterobacter spp. and CoNS (each 4.9%), P. mirabilis and Enterococcus spp. (each 2.5%).
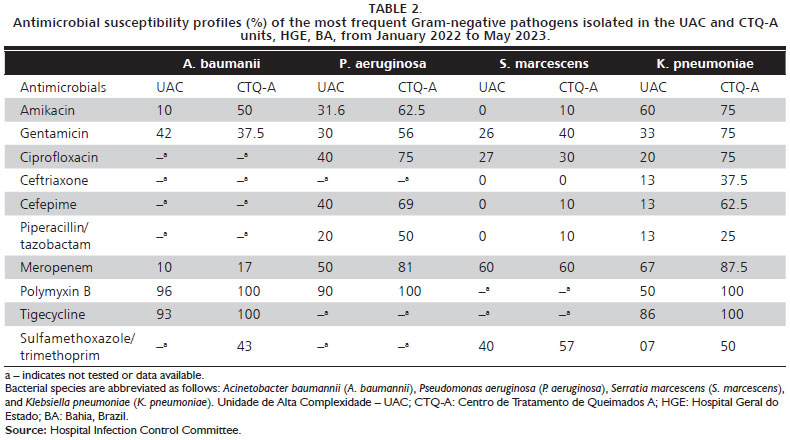
About the susceptibility of the isolates: it showed that 73.0% of the isolates in the UAC were classified as multidrug-resistant (MDR), in comparison to 50.0% of the pathogens in the CTQ-A. Among Enterobacterales, extended-spectrum beta-lactamase (ESBL) production was 62.0% in UAC and 54.0% in CTQ-A, while carbapenem resistance was 53.0% and 25.0%, respectively. Table 2 presents the antimicrobial susceptibility profiles of the most prevalent Gram-negative bacteria divided per ward. Among S. aureus isolates, the Methicillin-resistant S. aureus (MRSA) rate was 66.7% in UAC and 50.0% in CTQ-A.
DISCUSSION
This study provides an overview of ATB consumption patterns in two distinct burn units. DDD values varied considerably between the two units, with Meropenem (560 in UAC and 149 in CTQ-A), Vancomycin, and Teicoplanin being the most frequently used antibiotics.
Analysis of ATB consumption highlighted the high usage of Meropenem, which was the most prescribed drug in both units. This poses a dilemma as both units exhibit elevated rates of resistance to Meropenem, with A. baumannii generally showing less than 20.0% susceptibility. Additionally, the indiscriminate use of Meropenem contributes to selective pressure on P. aeruginosa and A. baumannii, two of the most prevalent pathogens in these units. To mitigate this issue, potential strategies include the use of Ertapenem for ESBL infections to reduce selective pressure on non-fermenting Gram-negative bacilli such as Pseudomonas and Acinetobacter, and the implementation of de-escalation protocols, which may involve switching to alternative antibiotic classes (e.g., quinolones), when clinically appropriate.
Regarding Gram-positive bacteria, we observed an excessive use of Gram- positive coverage, specifically Glycopeptides such as Teicoplanin and Vancomycin, in the UAC (intensive unit), despite Gram-positive pathogens accounting for only 17.0% of its isolates. To address this, we plan to implement targeted educational interventions for clinical staff to reduce the over-reliance on empiric Gram-positive coverage. Notably, during the study period, a 2-month shortage of Teicoplanin led to its substitution with Daptomycin or Linezolid (data not shown).
In contrast, 46.0% of the pathogens isolated from CTQ-A were Gram-positive, with Methicillin-sensitive S. aureus (MSSA) representing 14.0% of all isolates in this unit. However, the consumption data does not include Oxacillin and Cefazolin, the recommended agents for treating MSSA, which limits a full assessment of antibiotic use for this pathogen.
Other drugs, such as Sulfamethoxazole/trimethoprim, Ceftazidime/avibactam, Ceftolozane/tazobactam, Amikacin, and Gentamicin were not administered. The unit encourages their use when indicated, followed by monitoring of outcomes. During the analysis, we observed an opportunity to increase the use of Ciprofloxacin, as the susceptibility of most pathogens to Ciprofloxacin is often superior to that of Cephalosporins. Ceftazidime/avibactam and Ceftolozane/tazobactam are new drugs labelled as high cost in our service, for that reason their use only began in 2023 also their prescription is restricted and must be authorized by our infectious diseases specialist on call only for infections caused by MDR pathogens, guided by antibiograms and in the absence of other therapeutic options. That's why we have no available data on their use, yet.
The use of Ampicillin/sulbactam was considered suitable, because it is particularly indicated for Enterococcus spp. and A. baumannii, and its consumption aligns with the identification of these bacteria. However, it is important to note that higher doses are used in the treatment of A. baumannii.
Overall A. baumannii, P. aeruginosa, S. marcescens, and K. pneumoniae were the most prevalent pathogens in the UAC, whereas S. aureus, P. aeruginosa, and coagulase-negative Staohylococci prevailed in CTQ-A during the study period. The highest rate of MDR (73.0%) was observed in the UAC group.
This study has several limitations. As a retrospective analysis, it did not capture all ATBs used in the unit because it did not analyze the use of simpler antibiotics such as Oxacilin or Cefazolin. and some agents administered at loading doses or at higher than standard doses may have affected the accuracy of the DDD-based interpretations. This was a study based on general data from the unit, without focusing on individual patient data, meaning it was not possible to assess de-escalonation, mortality or treatment efficacy outcomes. Despite these drawbacks, we plan to continue monitoring ATB consumption and comparing trends within units over time. Notably, we found no published data on DDD consumption in other burn units in Brazil, highlighting the need for further studies aimed at burn patients. And from this, we can enable more detailed study designs to better understand outcomes.
CONCLUSIONS
At our center, DDD monitoring is integrated with a microbiological surveillance system, enabling the identification of treatment nonconformities in patients with burn injuries. Sharing these data will facilitate a broader discussion about the specific needs of this patient population. Regular analysis of antibiotic consumption supports the identification of areas requiring adjustment and contributes to the development of public health policies aimed at optimizing care and minimizing complications in patients with burn injuries.
ACKNOWLEDGMENTS
The authors would like to thank the Hospital Infection Control Committee (CCIH) and the medical coordination of the Burn Treatment Center (CTQ) for their support and encouragement throughout the development of this research. We also acknowledge the collaboration and logistical assistance provided by the Clinical Pharmacy and Laboratory Coordination teams of the institution, which were essential for data access and technical discussions during the study.
REFERENCES
1. Dai T, Huang YY, Sharma SK, Hashmi JT, Kurup DB, Hamblin MR. Topical antimicrobials for burn wound infections. Recent Pat Antiinfect Drug Discov. 2010;5(2):124-51.
2. Tiwari VK. Burn wound: how it differs from other wounds? Indian J Plast Surg. 2012;45(2):364-73.
3. Rowan MP, Cancio LC, Elster EA, Burmeister DM, Rose LF, Natesan S, et al. Burn wound healing and treatment: review and advancements. Crit Care. 2015;19:243.
4. Jeschke MG, Finnerty CC, Shahrokhi S, Branski LK, Dibildox M; ABA Organization and Delivery of Burn Care Committee. Wound coverage technologies in burn care: novel techniques. J Burn Care Res. 2013;34(6):612-20.
5. Branski LK, Mittermayr R, Herndon DN, Norbury WB, Masters OE, Hofmann M, et al. A porcine model of full-thickness burn, excision and skin autografting. Burns. 2008;34(8):1119-27.
6. Tyson AF, Boschini LP, Kiser MM, Samuel JC, Mjuweni SN, Cairns BA, et al. Survival after burn in a sub-Saharan burn unit: challenges and opportunities. Burns. 2013;39(8):1619-25.
7. Agbenorku P. Burns functional disabilities among burn survivors: a study in Komfo Anokye Teaching Hospital, Ghana. Int J Burns Trauma. 2013;3(2): 78-86.
Recebido em
3 de Setembro de 2025.
Aceito em
9 de Janeiro de 2026.
Local de realização do trabalho: Hospital Geral do Estado da Bahia (HGE), Salvador, BA, Brasil.
Conflito de interesses: Os autores declaram não haver.
![]() © 2026 Todos os Direitos Reservados
© 2026 Todos os Direitos Reservados
 Inglês PDF
Inglês PDF Imprimir
Imprimir
 Enviar este artigo por email
Enviar este artigo por email
 Como citar este artigo
Como citar este artigo
 Enviar um comentário
Enviar um comentário
 Mendeley
Mendeley
 Pocket
Pocket
